
At some point, there will be a revolt. The longer the arbitrary insanity persists, the more violent the reaction will be.
By Roger Kimball, AM GREATNESS
The most cheerful headline I have seen in weeks was on Glenn Reynolds’ New York Post column: “No, Karen, we’re not masking again.” I hope he is right. I do wonder, though. I have no doubt that the second part of his headline—“A winning GOP message for 2022 [and] beyond”—is correct. At least it’s correct if it is expressed as a conditional: It would be a winning strategy were it adopted. As Reynolds notes, “There is a great deal of pent-up frustration and resentment over the inconvenience, the loss of freedom and the general climate of hectoring that the government’s pandemic response has created.” Indeed. And he’s right, too, that;
It’s irritating to be lectured by officials who claim to be smarter than you. It’s infuriating to be lectured by government officials who claim to be smarter than you—but clearly aren’t.
The on-again/off-again claims on masks and vaccination are just part of it. Tired of masks? Get vaccinated, they told us. Now they’re saying wear a mask, even if you’ve been vaccinated and even if you’re associating with others who’ve been vaccinated.
And there’s talk of more lockdowns, which a growing body of scientific evidence suggests were perfectly useless and downright harmful.
As Molly Bloom exclaimed in a different context, Yes, Yes, Yes!
But to return to the question of hope, I am reminded that hope was said by some cynics to have been the last evil in Pandora’s pithos. It seems like only yesterday—in fact, it was just this past May—that both the president and the vice-president of the United States insisted that (as Joe himself put it) “Folks, if you’re fully vaccinated—you no longer need to wear a mask.”
Of course, that was more than a year after “15 days to slow the spread,” Anthony Fauci’s steady stream of contradictory, though authoritatively delivered, advice, not to mention the recent advent of (cue the scary music) The Delta Variant.
It was the New York Post, again, that cut to the chase on the latest (unless we’re on to the epsilon variant already) with its cover of July 30. “Insanity!” read its oversized headline and below was a large grid with a tiny bit of the upper right square marked. Of the 161 million people who have been vaccinated, only 5,601 have been hospitalized with the new version of the virus. Of those, only 1,141 have died. That’s .0007 percent. (And how old, one wonders, were those who succumbed and from what comorbidities did they suffer?)
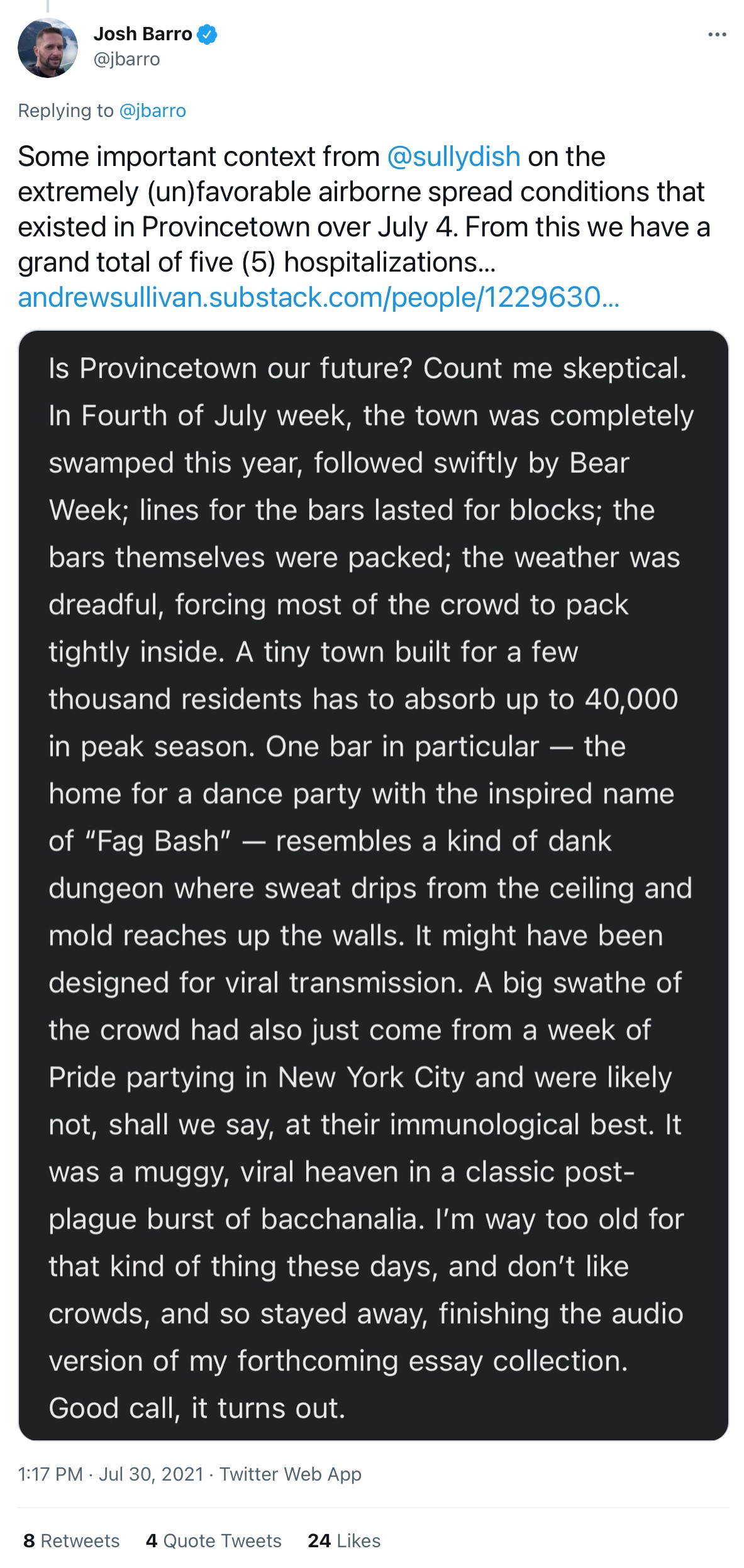
Now it turns out that the latest CDC advice was based largely on an outbreak at Provincetown after the informal party time of “Bear Week” in early July. Andrew Sullivan treated the news with some portion of the skepticism it deserves. In fact, as another commentator pointed out, what the Provincetown outbreak really shows is that “even under perfect conditions for a superspreader event, the vaccine works spectacularly well.”
But even to talk about studies and statistics and “expert” advice is to assume that we are talking primarily about an issue of public health. We aren’t. Consider this list from Jim Treacher:
- Absolutely do not wear a mask
- You must, must, must wear a mask or you’re killing Grandma
- Don’t leave the house or you’re killing Grandma
- If you can’t avoid leaving the house, stay at least six feet away from any other human being you see or you’re killing Grandma
- Wash your hands 20 times a day
- Do not touch your face or anything else, ever
- Get vaccinated so you don’t have to wear a mask
- You have to wear a mask even if you’re vaccinated
- When the above rules change, and then change back, and then change back again, shut up about it or you’re a stupid MAGA-head
- Don’t forget to vote Democrat!
Of course, the last item is more often left unspoken than it is overtly expressed, but it is a sentiment, an assumption, that infuses the whole shifting kaleidoscope of contradictory advice. Treacher is right. “This isn’t about science. It’s about control. You will do as you’re told, peasants, and your moral, ethical and intellectual betters will continue to do whatever they please.”
I think Glenn Reynolds is correct that opposing the tyrannous spirit that stands behind the lockdowns, the mask mandates, and the smug, hectoring, politically correct demands for proof of vaccination would be a winning strategy for GOP politicians. Will they adopt it? Most will do so timorously, if at all. That’s my prediction.
Last year at Encounter Books, we published an admonitory book by Joel Kotkin called The Coming of Neo-Feudalism: A Warning To The Global Middle Class. Some people thought Kotkin was overstating things with his talk of an increasingly stratified society in which a tiny elite lorded it over an increasingly pauperized and disenfranchised mass. It turns out, though, that if anything Kotkin understated the trends. The weaponization of public health diktats, their enforcement by a vast and increasingly overbearing cadre of nanny-state bureaucrats, is simply the latest manifestation of the profoundly anti-democratic spirit that has taken hold in Western societies.
It’s all about social control, as Jim Treacher says. At some point, there will be a revolt. The longer the arbitrary insanity persists, the more violent the reaction will be. The question is whether we are at or are approaching the point of crisis. Will the voters stand for another lockdown as we approach the 2022 election? Lockdowns markedly increased the opportunities for voter fraud; 2020 showed that. That is precisely why the swamp is prepping us for another go. Let’s see if we stand by grumbling impotently or if, finally, we actually do something. I am not holding my breath.
<
>


{kind=link}
This is a very disturbing report from Yahoo news. Although the author does not say so and seems to be a naive epidemiologist-in-training, I think the article reveals how medical researchers may have “developed” SARS-Cv2-19, and how they are working on developing new “animal-to-human deadly diseases.
Epidemiologists who detect animal viruses that have “jumped” or have the potential to jump to humans can then use “evolutionary theory” to do “gain-of-function” work in a laboratory, and leak them into the human environment, thereby making a fortune for drug companies funding this research and advancing Bil Gates’ population-control agenda. Some of the young epidemiologists-in-training may assist in this virus-development process without knowing how they are being used by their “experienced” supervisors.